The MRCT Center hosted a 2-day hybrid meeting in Washington DC in October 2024 to examine the potential benefits, challenges, and opportunities of platform trials for pediatric populations. In addition to consideration of overarching issues, three diseases – pediatric oncology, major depressive disorder (MDD), and multidrug-resistant tuberculosis (MDR-TB) – were chosen to represent different conditions, epidemiology, settings, therapeutic challenges, and patient populations, and to illuminate different potential approaches and solutions.
With ~80 pediatric and platform trial experts from Europe, the UK, Asia, Australia and the US in attendance, the discussants were successfully identified knowledge gaps and practical challenges that impact pediatric platform trial planning and execution. Each of the three subgroups recommended actionable approaches to address identified issues, and the respective groups continued to meet and take concrete steps, furthering the momentum created at the workshop, with the MRCT Center remaining actively involvedwith each disease-specific subgroup to facilitate the next steps.
We appreciate the financial support of several companies, without whom this workshop would not have been possible. The workshop was supported in part by voluntary contributions from AstraZeneca, Johnson & Johnson, and Sanofi. Our thanks to all the individuals who contribute their time and expertise to the planning and conduct of this workshop and without whom this event would not have been possible. We are delighted to share the comprehensive workshop report, a detailed summary of the meeting proceedings.
Podcast Episode: Advancing Pediatric Platform Trials – A Conversation with Dr. Danny Benjamin
Recorded during the MRCT Center’s October 2024 conference, Advancing Pediatric Platform Trials: Streamlining Development, Maximizing Impact, this keynote conversation features Dr. Danny Benjamin, Kiser-Arena Distinguished Professor of Pediatrics at Duke University Medical Center.
Discussion Highlights:
The historical evolution of pediatric drug development and key regulatory milestones
The role and achievements of the Pediatric Trials Network (PTN)
How platform trials can increase efficiency and reduce burden in pediatric research
Ethical and operational challenges unique to pediatric platform trials
Real-world examples demonstrating the value of shared trial infrastructure
Future directions to drive innovation, collaboration, and regulatory alignment
Dr. Lembit Rago, Secretary-General of the Council for International Organizations of Medical Sciences (CIOMS), delivered a compelling keynote on CIOMS initiatives to define and synthesize professional competencies essential for clinical research and emphasized the importance of cooperative agreements to harmonize workforce development efforts.
The session also highlighted the Joint Task Force for Clinical Trial Competency (JTF) Framework as a foundational tool for training and professional development, addressing the challenges and opportunities in recruiting and retaining a diverse and capable workforce.
Sally Armstrong, CEO of PRAXIS Australia, shared how PRAXIS has incorporated the JTF Framework into their educational offerings—including courses, workshops, and immersive onsite training programs.
Susan Landis, Executive Director of the Association of Clinical Research Professionals (ACRP), discussed ACRP’s “Partners Advancing the Clinical Research Workforce” initiative, which uses the JTF Framework to support a diverse and qualified clinical research workforce through training programs, resources, and strategic collaborations.
A recording of the webinar and the presentation slides are available here:
A key aspect of health literacy—especially in clinical research—is understanding what data is collected, how it is protected, and how it is used during and after a study. Truly informed consent requires transparency about data practices so that participants can make educated decisions.
During this webinar we discuss the importance of data literacy, explore practical applications for research teams, and unveil new materials designed to support participants and the broader research community.
Key Topics:
Advancing Data Literacy as a Component of Health Literacy: Explore how understanding research data supports informed decision-making and aligns with broader health literacy efforts.
Applying Plain Language and Visual Tools to Data Communication: Learn how the MRCT Center and PHUSE have used plain language and infographics to make clinical research data more accessible.
Empowering Participants with Transparent and Actionable Information: Identify ways to integrate data literacy resources into your clinical research processes to support research trust and engagement.
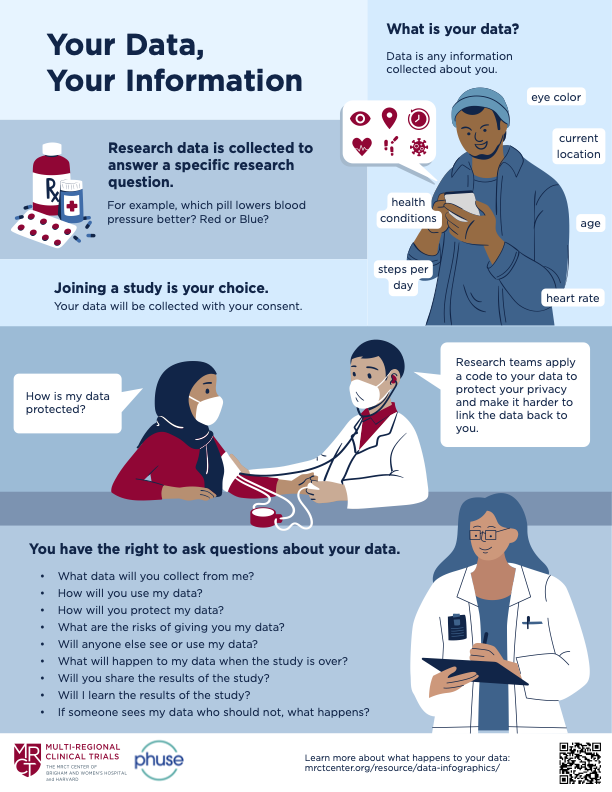
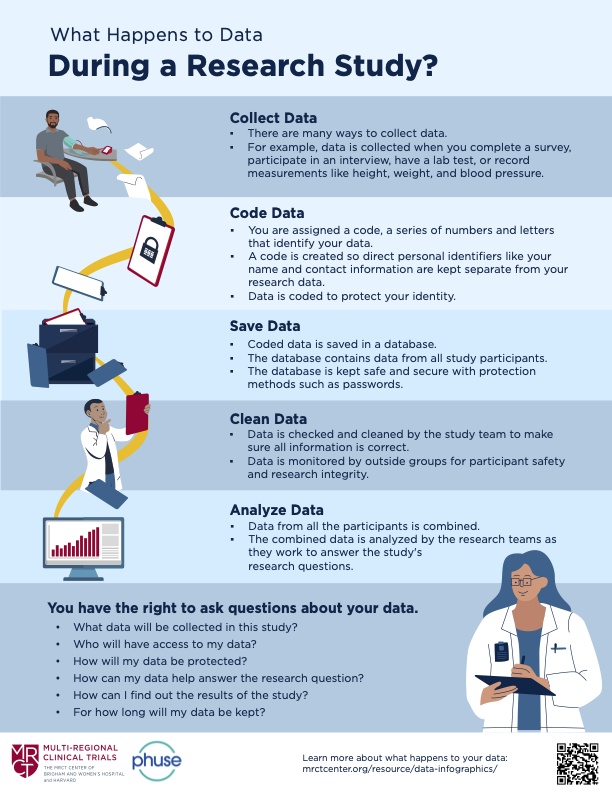
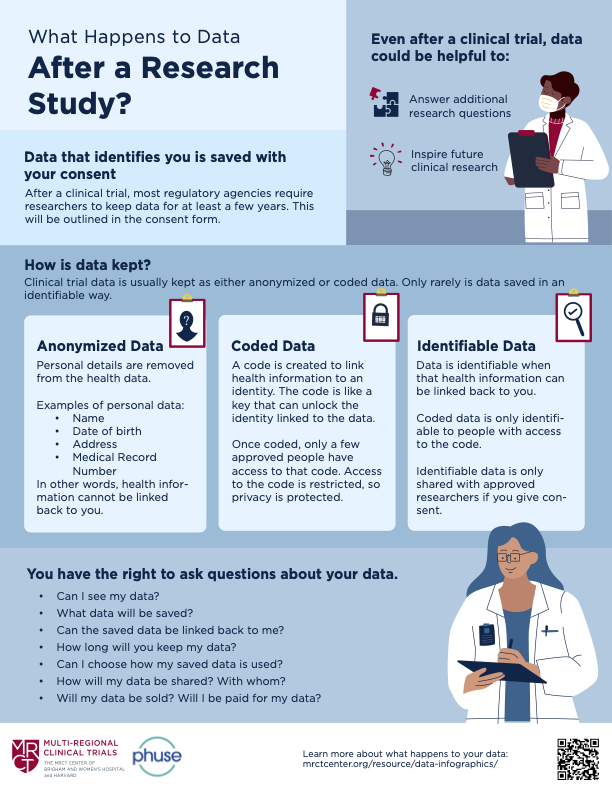
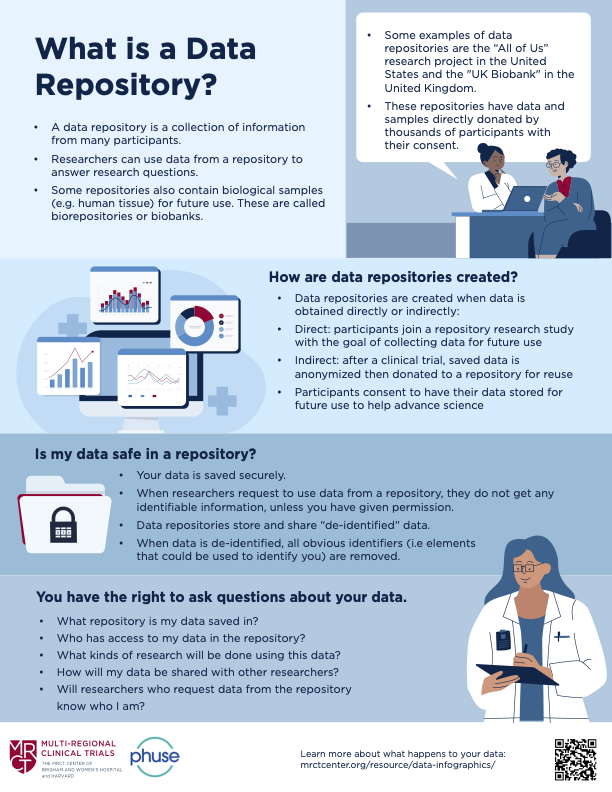
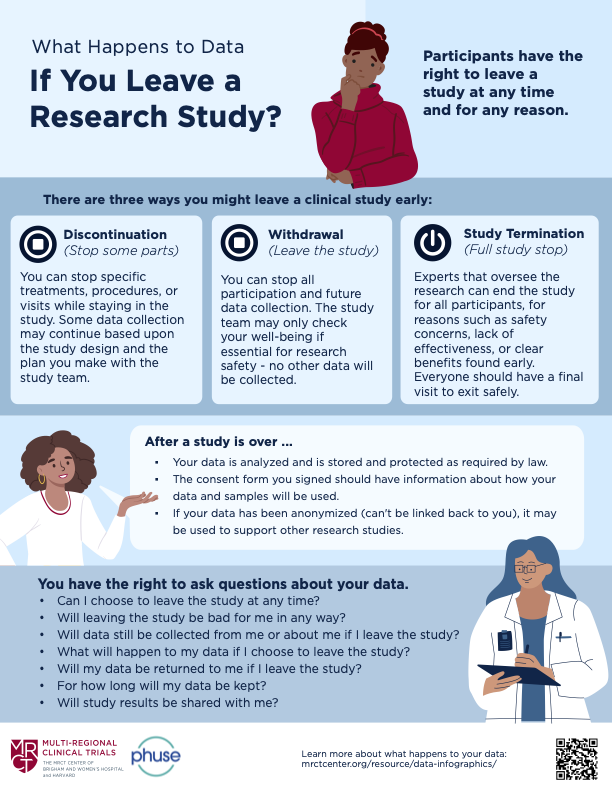
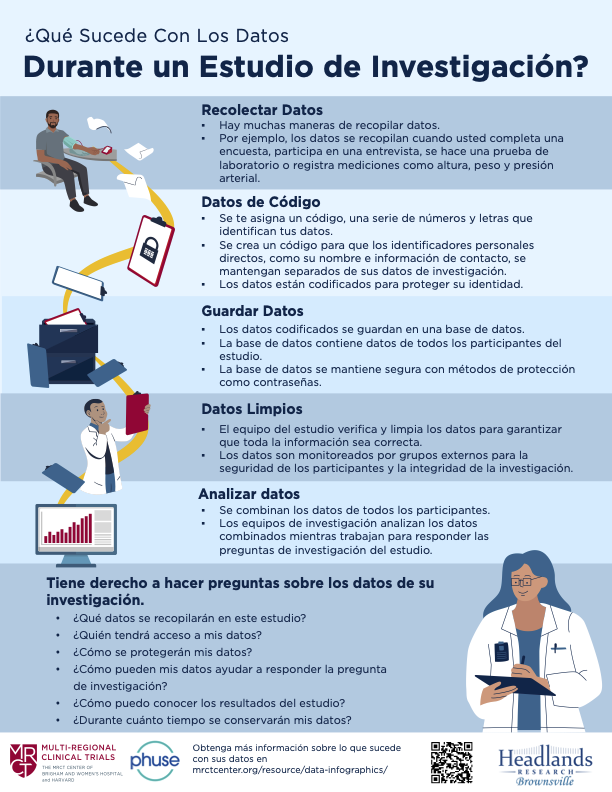
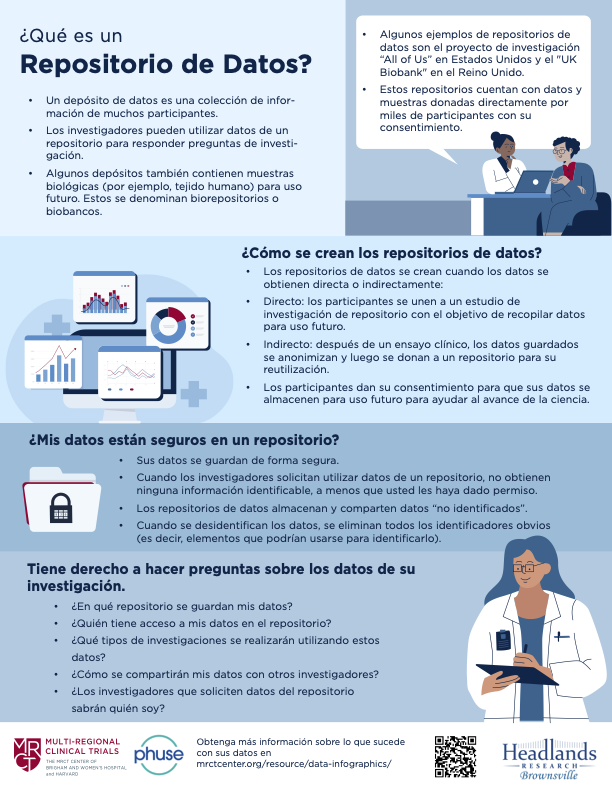
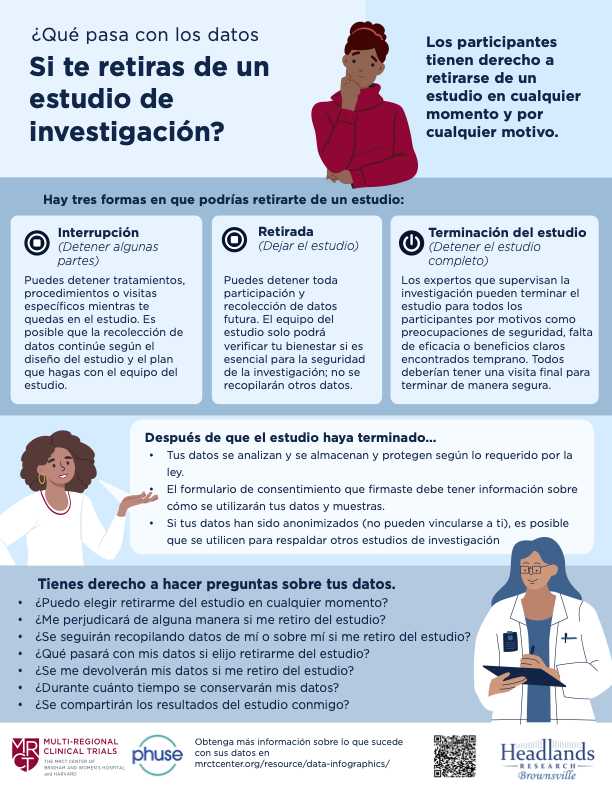
The MRCT Center is pleased to collaborate with the PHUSE Data Transparency team on materials to educate the general public on Data Privacy and Data Sharing. These materials were presented at a webinar on April 3, 2025. The recording and slides are now available on-demand here.
These infographics and videos are freely available and designed to explain how data is used and protected in clinical research.
Disabled people are often excluded from health research despite being the largest underserved group in many countries, having worked to enshrine legal mandates for fair treatment and equal opportunity, and driving innovations that benefit everyone. The article describes the research cycle, points at which disabled people currently face barriers, and actions that can be taken by the research community to better involve disabled people during those points in the research cycle. This call to action is made by authors from different countries around the world as part of the Disability Inclusion in Research Collaboration (DIRECT) to emphasize the critical importance of collaboration, learning, and support across countries on this issue.
The MRCT Center, on behalf of the Convergence Project hosted a virtual event focused on workforce development strategies to support a more dynamic and competitive clinical research workforce. This meeting brought together community leaders, policymakers, and researchers to discuss how to create and support pathways into the clinical trial workforce (e.g., part-time degree programs, community colleges, fellowships). Key topics included workforce development, targeted recruitment, and actionable steps to drive systemic improvements, and meeting attendees had the opportunity to pose questions to panelists leading programs in Georgia, North Carolina, South Dakota, and other states across the country.
Capacity strengthening is vital to ensure that countries—particularly those with limited resources—can conduct effective, high-quality clinical research. The ability to perform rigorous trials is often constrained by inadequate infrastructure, regulatory processes, and a lack of trained researchers. As noted by the Science for Africa Foundation, despite accounting for over 25% of the global disease burden, Africa hosts only about 4% of global clinical trials. To address these gaps, supporting locally-driven capacity-building initiatives is key. This involves collaborating with national health departments, research institutions, and local communities to create sustainable, long-term systems that enhance both healthcare and research capabilities.
Capacity-building efforts can be approached at three levels: individual, organizational, and national. These include fostering researcher skills, improving research infrastructure, and strengthening the national regulatory environment. It is essential to work with local stakeholders to identify needs and design solutions that will be effective long term. For example, external funders can support training opportunities for local researchers, enhance regional collaboration, and promote community engagement to raise awareness of clinical research. By taking a comprehensive, staged approach to capacity strengthening, we can build resilient research systems that ultimately lead to more inclusive healthcare innovation and a more equitable global research landscape.
Embedding Ethical Considerations Relating to Global Representation in Clinical Research offers a thorough exploration of the ethical issues surrounding global representation in clinical trials. Central to the document is the ethical imperative to ensure that clinical research reflects the populations most affected by the diseases being studied while addressing the systematic inequalities that limit access to participation. The guide raises key ethical questions: Are the right groups being included in the research? How can we ensure that participants will benefit from the outcomes, both during and after the study? How are diverse populations, particularly in low-resource settings, engaged ethically and without exploitation?
This document also provides a valuable framework for study sponsors and research teams, offering a series of ethical considerations and questions that should be addressed throughout the study process. These considerations include the need for thoughtful engagement with local communities, careful assessment of barriers to participation, and strategies to reduce the risk of exploitation or undue inducement. By documenting their responses to these ethical questions, sponsors and study teams can ensure that their studies are conducted with integrity, fairness, and respect for all participants, helping to create research that is not only scientifically valid but also ethically sound and globally representative.
Comments provided to: U.S. Food and Drug Administration; FDA-2024-D-4245
Description: The MRCT Center commented on the FDA’s draft guidance, Study of Sex Differences in the Clinical Evaluations of Medical Products, advocating for the use of real-world data (RWD) and real-world evidence (RWE) to support post-marketing evaluations of sex differences, inclusion of intersex and transgender individuals, additional guidance on the inclusion of pregnant and lactating individuals, and further advice on statistical approaches to detect sex-based differences.
Comments provided to: U.S. Food and Drug Administration; FDA-2024-D-2402
Description: The MRCT Center’s public comments on the FDA’s draft guidance, Considerations for Including Tissue Biopsies in Clinical Trials, recommend enhanced clarification on biopsy justification, prioritization of less invasive methods, consent specificity for future research, and strengthened IRB considerations to improve ethical rigor and participant protections.