

You need to be logged in to view this content. Simple Membership is not configured correctly. The login page or the join us page URL is missing in the settings configuration. Please contact Admin
Focus Area: Clinical Trials & Research
DIA Clinical Trial Data Sharing
Presentation
Presented on: September 18, 2015
Published at: DIA Meeting on Clinical Trial Disclosure & Data Transparency, Bethesda, Maryland
MRCT Center Transitioned to the Division of Global Health Equity
As of July 1, 2015, the MRCT Center has moved administratively to the Division of Global Health Equity, under the leadership of Dr. Paul Farmer, at the Brigham and Women’s Hospital (BWH), a Harvard teaching hospital. The Division of Global Health Equity serves as an academic and research home for more than 40 Harvard and BWH faculty who are engaged in teaching, patient care and research around the world and domestically.
The integration of the MRCT Center into the Division offers a community of colleagues and a network of thought leaders globally, as well as infrastructure for program strengthening and expansion. The mission of the MRCT Center will remain unchanged and will be strengthened through this new partnership. The MRCT Center will continue to have a collaborative relationship with Harvard, including the continued involvement of multiple Harvard faculty members and student interns.
In the process of this move, the URL of the MRCT Center’s website changed to: mrctcenter.org, and our email addresses changed to @MRCTcenter.org. Web searches and emails to previous addresses will be redirected. The general email box for the center is admin@MRCTcenter.org. Our full name is now: The MRCT Center of Harvard and Brigham and Women’s Hospital.
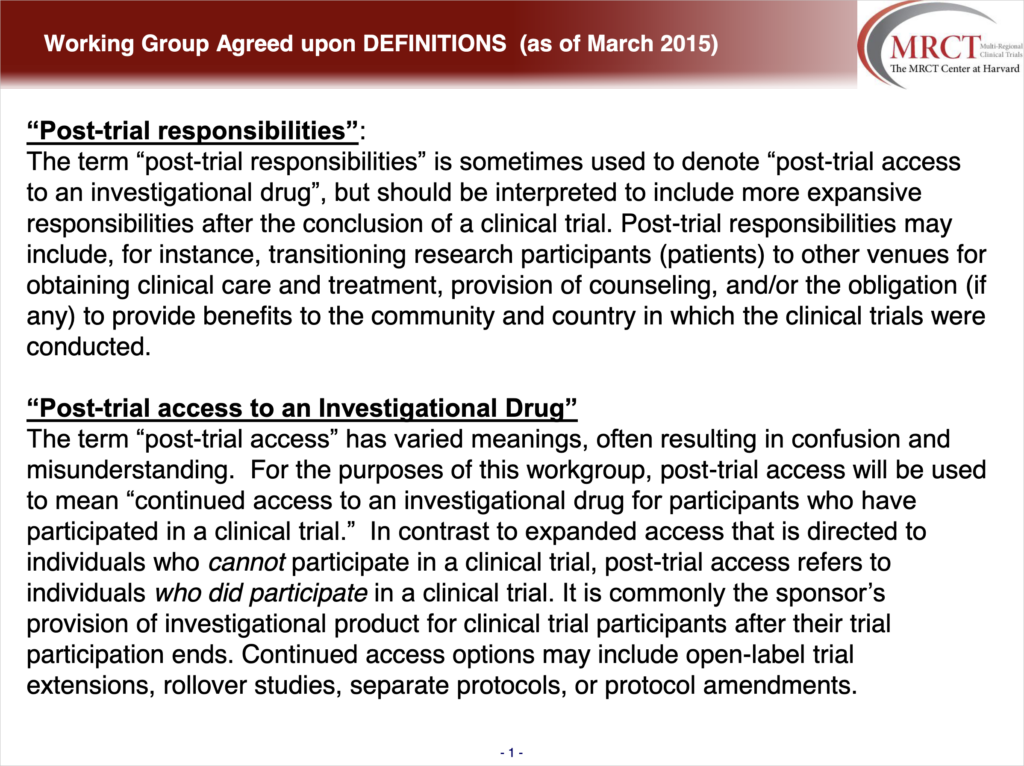
Post-Trial Responsibilities Defined
March 15, 2015
The Post-Trial Responsibilities Working Group, sponsored by the MRCT Center at Harvard, was launched in February 2015 and is a multi-stakeholder group with 55 members from academia, industry, non-profit organizations, government, and patient organizations. Twelve countries are represented.
The purpose of this working group is to develop an ethical framework for post-trial responsibilities, including case studies and practical guidance, which can then be used to conduct training sessions.
As an initial step, the working group focused on a single consensus definition of post-trial responsibilities and related terminology – post-trial access to an investigational drug, and expanded access of an investigational drug. These definitions will serve as the platform upon which the framework will be based. The consensus definitions as of March 2015 can be accessed below.
Global Clinical Trials: Ethics, Harmonization and Commitments to Transparency
Publication
Published on: April 29, 2015
Published in: Harvard Public Health Review
Improving ethical issues in clinical trials in developing countries
There are multiple ethical challenges for conducting multi-regional clinical trials in developing countries, such as whether patients in developing countries are free to participate in research if access to essential medicines is tied to research, and how informed consent can be assessed and risks and benefits understood when the element of choice is so different.
The MRCT Center has developed an Essential Ethics Toolkit and E-Learning course that address these and other issues and is committed to transparency, dissemination, and harmonization.
Read more about this in: “Global Clinical Trials: Ethics, Harmonization and Commitment to Transparency,” published in Volume 5 of Harvard Public Health Review.
MRCT Post Trial Responsibilities Conference Proceedings Available
September 18, 2014
MRCT Center at Harvard collaboratively with the Petrie-Flom Center for Health Law Policy, Biotechnology, and Bioethics at Harvard Law School hosted a one-day open conference on post-trial responsibilities on September 18, 2014, at the Harvard Law School.
The objectives of the conference were to discuss implications of international guidance on post-trial responsibilities for clinical research, to articulate and understand the range of perspectives on post-trial responsibilities, to draw lessons from successful and unsuccessful attempts to implement post-trial policies, and to discuss potential scenarios and practical solutions for post-trial responsibilities that may inform policy in this important area moving forward.
Presentations:
VIDEOS
A Conference on Post-Trial Responsibilities: Ethics and Implementation
Proceeding
Proceedings from MRCT Center at Harvard Post-Trial Responsibilities
Conference on: Sept 18, 2014
Held at: Harvard University
Harvard MRCT Post Trial Responsibilities Conference Session 4
Harvard MRCT Post Trial Responsibilities Conference Session 3
Presentation
Presented on: Sept 18, 2014
Presented at: Harvard Post-Trial Responsibilities Conference